{kind=link}
A recent study shows that for colon cancer patients over 75, tailoring treatment based on cancer stage and risk factors, rather than automatically scaling back, can boost survival rates. This finding challenges the notion of withholding treatment solely due to advanced age.
Researchers from Seoul St. Mary’s Hospital, led by Dr. Lee Yoon-seok of the Colorectal Surgery Department, announced on Monday their analysis of adjuvant chemotherapy’s effectiveness in elderly colon cancer patients. Their results underscore that treatment strategies based on cancer stage and risk factors, not age alone, are key to improving survival rates.
This groundbreaking study earned the Best Poster Award at last year’s American Society of Colon and Rectal Surgeons (ASCRS 2025) conference, garnering praise for offering evidence-based treatment guidance to previously hesitant patients.
Colon cancer, the third most common cancer globally, affects over 1.9 million people annually. Of the 32,610 colorectal cancer cases, colon cancer accounts for 17,103 (52.4%), with about a third (5,944 or 34.8%) occurring in those 75 and older.
Given that colon cancer is often diagnosed at advanced stages, post-surgery adjuvant chemotherapy is crucial for preventing recurrence. However, concerns about elderly patients’ physical condition, potential side effects, and lack of clear clinical data have created dilemmas for healthcare providers, patients, and families alike.
To address this, Dr. Lee’s team analyzed data from 1,585 colon cancer patients who underwent radical resection across five Catholic Central Medical Center hospitals. They focused on 394 patients aged 75 and older, finding that only 184 (46.7%) received adjuvant chemotherapy.
The team noted this figure is roughly half the 87.9% chemotherapy rate for patients under 75, indicating a clear hesitancy in administering chemotherapy to elderly patients.
To assess chemotherapy’s effectiveness, the researchers divided the 394 elderly patients into three groups: high-risk stage II (164 patients), low-risk stage III (108 patients), and high-risk stage III (122 patients). The most significant benefits were observed in the high-risk stage III group.
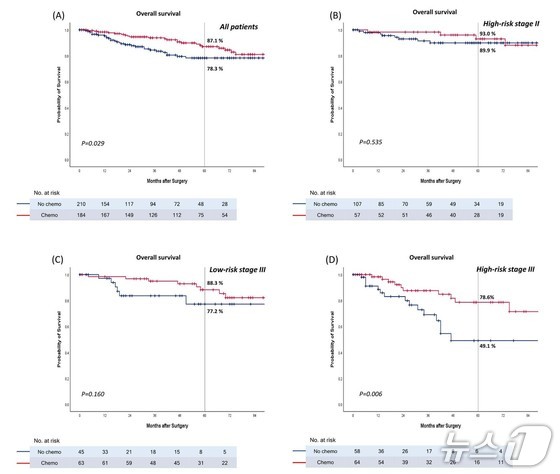
For high-risk stage III elderly patients, chemotherapy boosted the five-year overall survival rate to 78.6%, a remarkable 29.5 percentage point improvement over the non-treatment group (49.1%). Moreover, the five-year disease-free survival rate, a critical measure of cure, jumped from 48.2% to 69.3%.
The benefits were less pronounced in the high-risk stage II and low-risk stage III groups, highlighting the need for personalized treatment strategies rather than a one-size-fits-all approach for elderly patients.
Dr. Lee emphasized that this study provides compelling evidence that chemotherapy significantly enhances survival rates in specific high-risk groups. It hopes it will mark a turning point, encouraging more proactive treatment decisions for elderly patients, rather than automatically ruling out options based on age alone.
Lead author Dr. Bae Jeong-hoon added that the essence of medical care is maximizing treatment effectiveness by carefully weighing the tangible benefits for each patient. The findings show that even high-risk stage III elderly patients can reasonably expect both extended life and improved quality of life with appropriate treatment.
Colon cancer treatment varies by stage: Stage I can often be cured through endoscopic or laparoscopic resection, stages II and III typically require post-surgery adjuvant chemotherapy to prevent recurrence, while stage IV calls for chemotherapy, targeted therapy, or surgical removal of liver or lung metastases.